


Introduction
In a multicenter survey of 6 hospitals in the Republic of Korea (ROK) on a given day, malnutrition was observed in 20.2% (n = 99 patients) of hospital admissions [1]. Undernourishment in admitted patients increases the mortality rate, length of hospital stay and economic burden [2,3]. Having a Nutrition Support Team (NST) has been shown to have a positive effect on the supply of nutrition to critically ill patients and reduce the length of hospital stay [4ŌĆō6]. In ROK, the need for a NST emerged in the 1990s, and NST activities were carried out in earnest within hospitals from the 2000s. However, many attending physicians do not comply with NST advice [7,8]. Therefore, the objective of this study was to investigate the compliance of attending physicians with the NST advice and its effect on the outcome of treatment for critically ill patients. This study was performed in a single university medical institution.
Material and Methods
Data were collected retrospectively using electronic chart reviews from March, 2015 to August, 2016. Patients who were more than 18 years but less than 90 years, had been admitted and managed in the intensive care unit (ICU) were studied. Of these patients, readmission cases and mortality cases within 2 weeks were excluded. The clinical characteristic data such as age, gender, weight, body mass index, Acute Physiologic Assessment and Chronic Health Evaluation II (APACHE II) score, nutritional status, and laboratory findings (albumin, total protein, hemoglobin, lymphocyte count, and glucose levels) were retrieved.
Nutritional strategies including the total total calories and protein requirements calories and protein requirements were determined using the ASPEN guidelines. A simplistic weight-based equation was used to determine the calorie requirement (25ŌĆō30 kcal/kg/d), and protein requirement (1.2ŌĆō1.5 g/kg/d). Malnourished patients were assessed using the International Classification of Diseases, 9th revision, Clinical Modification (ICD-9-CM) with malnutrition described as mild, moderate, or severe [6]. In this study nutrition was categorized as good, mild malnutrition, moderate malnutrition, or severe malnutrition.
The NST was involved in clinical support for nutrition when the attending physician requested a consult regarding a patient in the ICU. Patients in this study were assigned to a group depending on the primary physicianŌĆÖs compliance with the NST recommendations. For the group whose attending physicianŌĆÖs compliance with the NST advice was good, it was named the ŌĆ£compliance group.ŌĆØ The group whose attending physician did not follow the recommendations from the NST was called the ŌĆ£non-compliance group.ŌĆØ Compliance was judged using several factors such as the time taken to initiate nutrient support (early vs. late initiation), supply methods (enteral nutrition vs. parenteral nutrition), the number of calories supplied (increased vs. decreased), the amount of protein supplied (increased vs. decreased), following recommendation for using a feeding pump, treatment for refeeding syndrome, and problems with defecation. After the consultation, if the attending physician followed the NST recommendations mentioned above, the patient was assigned to the ŌĆ£compliance-group.ŌĆØ Compliance was judged by a multidisciplinary team during the ICU rounds once a week. Outcomes including 30-day mortality, overall mortality, duration of ICU stay, duration of hospital stay, and duration of ventilation days were compared between the 2 groups (compliance vs non-compliance) as well as several nutritional variables (total number of calories supplied, total protein supply, nutritional methods, and nutritional laboratory variables) and demographics.
Nutritional variables and laboratory findings 14 days later were also compared between the 2 groups at the time of consultation and according to compliance. Survival curves were also compared beyond 1 year according to the compliance. Patients who had died within 2 weeks after consultation were excluded from analysis because it was thought that factors other than nutritional issues were the cause of mortality.
Analysis was performed using SAS Version 9.4 (SAS inc., Cary, NC, USA). Chi-square tests and t tests were performed to determine characteristics of all patients studied. Statistical uncertainty was expressed as 95% confidence interval. Probability values which were < 0.05 were considered statistically significant.
The protocol of this study was approved by an independently constituted ethics committee within the institution (ethics approval no.: CR 318074).
Results
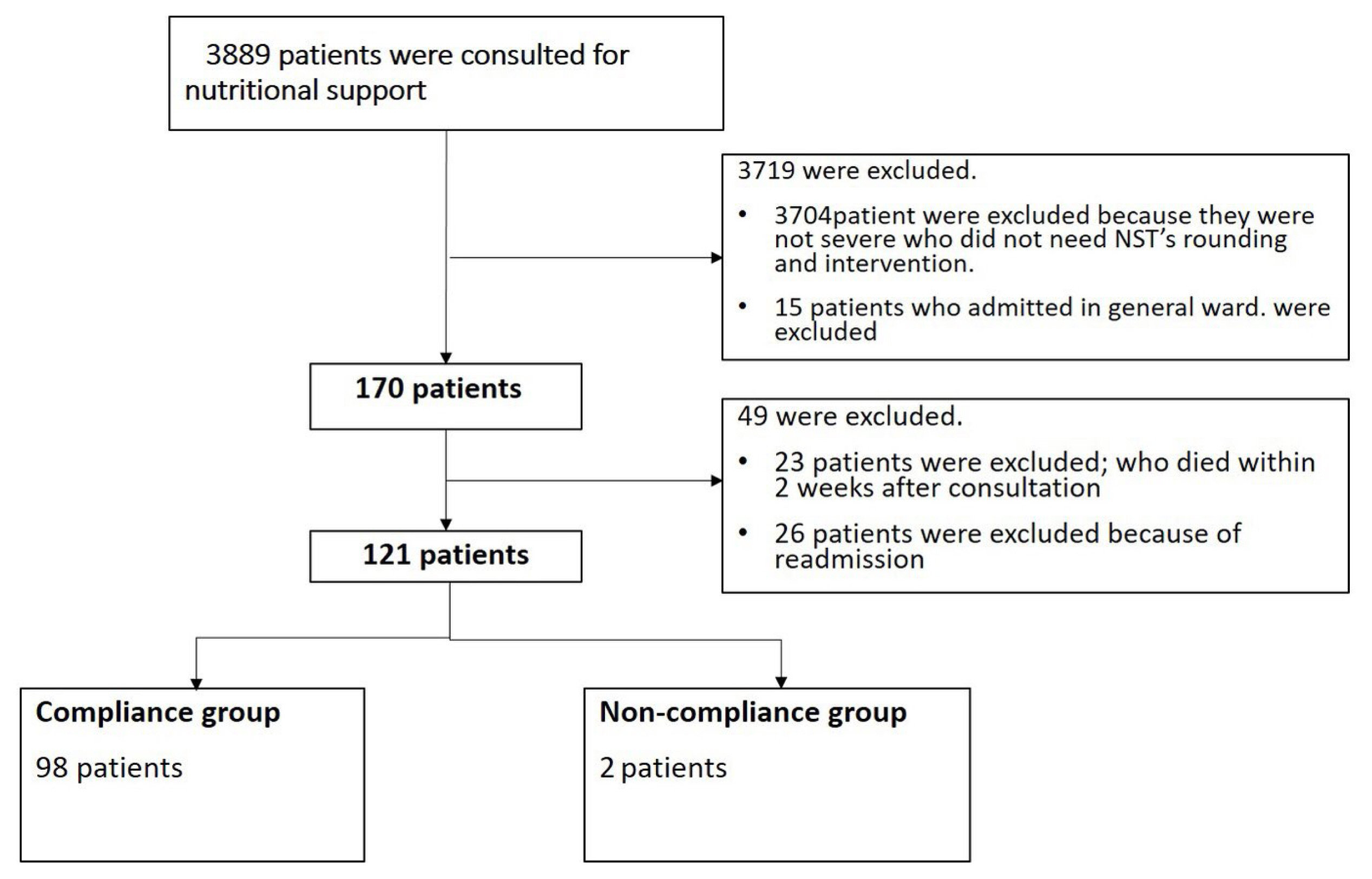
A total of 170 critically ill patients who stayed in the ICUs of a single hospital was retrospectively studied. The involved ICUs are surgical, trauma, neurosurgical, medical, and emergency ICUs. Of these patients, readmission cases (n = 26) and mortality cases (n = 23) within 2 weeks of admission were excluded from this study. Consequently, 121 patients were analyzed in this study (Figure 1; Table 1). The mean APACHE II score of these 121 patients was 15.91 (minimum 2, maximum 44). More than 80% of these patients had malnutrition (mild, 32.2%; moderate, 28.9%; and severe, 19%).
On the 14th day after the consultation with the NST, the average supply of calories and protein increased for the study group of patients in the ICU (calories: 230.11 ┬▒ 651.04 kcal, p < 0.01; protein: 9.45 ┬▒ 36.97 g/day, p < 0.01). After consultation, these calories and protein supplies were ranked as 75.9% and 75.6% of the calculated requirement, individually. Laboratory findings including total protein, albumin, glucose, and CRP levels became more stable on the 14th day after the NST consultation. The case of enteral nutrition increased more (n = 19 pre-consultation and n = 30 post consultation) than that of parenteral nutrition (n = 54 pre-consultation and n = 29 post consultation) (Generalized McNemar and BhapkarŌĆÖs test, p < 0.01; Table 2).
For comparison between the compliance group and the non-compliance group, there was no significant difference in basic demographics. The compliance group showed a better outcome in the 30-day mortality rate (8% vs. 26%, p = 0.02). For the overall mortality rate, the compliance group showed a lower mortality rate, however this was not statistically significant (21% vs. 39%, p = 0.08; Table 3). When nutritional variables were compared prior to and following the consultation with the NST and in both the compliance and non-compliance groups, the total calories (1,146.36 ┬▒ 473.45 kcal vs. 832.45 ┬▒ 364.28 kcal, p < 0.01) and protein (55.00 ┬▒ 22.30 g/day vs. 42.98 ┬▒ 24.46 g/day, p = 0.04) supplied were significantly more in the compliance group compared with the non-compliance group. After the consultation, the compliance group was supplied 79.7% of required calories and 79.1% of the required amount of protein, which were individually higher than the non-compliance group (59% of the required calories and 60.5% of the required amount of protein). Parenteral nutrition was the main method of supply in both groups before the consultation (n = 43 in the compliance group and n = 11 in the non-compliance group). However, the prevalence was lower in the compliance group after the consultation (n = 17 in the compliance group and n = 12 in the non-compliance group; Chi-square test, p < 0.01; Table 4).
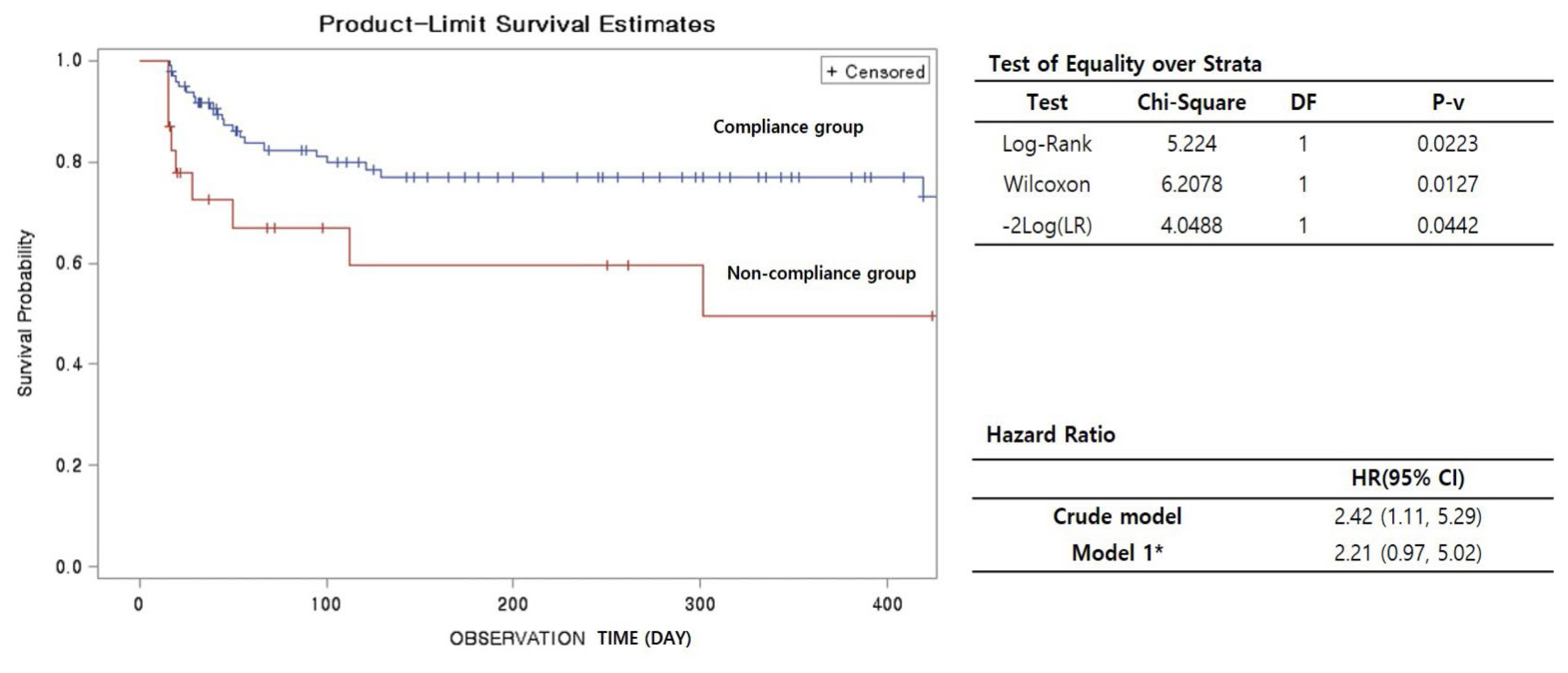
When survival rates of patients were estimated beyond 1 year after the consultation with the NST, the survival rate was higher in the compliance group than the non-compliance group (Crude Model; hazard ratio: 2.42, 95% CI: 1.11, 5.29). The survival rate remained higher in the compliance group after adjusting for age, gender, weight, and APACHE II score (hazard ratio: 2.21, 95% CI: 0.97, 5.02; Figure 2).
Discussion
Nutritional support has been recognized as an important strategy for the treatment of patients in the ICU. Many for parenteral and enteral nutritional developments have been accomplished in the world [2,3]. For approximately 4 decades, many physicians have known that the NST is important in achieving nutritional goals in terms of calories and protein for patients in the ICU [9ŌĆō11]. In 1986, it was anticipated that NST polices would be expanded to encourage greater utilization of the NST [12]. However, the NST system in Korea is not in full operation yet. In the cases where the NST were consulted it depended on the attending physicianŌĆÖs decision to follow the recommendations. Non-standardization of nutritional strategies may induce malnourishment or worsen it and this correlates with a bad treatment outcome [2,3,13,14]. The NST plays an important professional role in introducing information and suggesting alternative methods of nutritional support. The NST is a multidisciplinary team that has a positive effect on sufficient patient calorie supply, reducing the incidence of parenteral nutrition, and associated induced infections [2,3,10,15,16]. In the ROK, the government began support for the medical charge of the activity of the NST in August 2014. Its activity also became an appraisal standard for tertiary hospital evaluations. However, the potential effect of the NST advice could be immaterial without physiciansŌĆÖ compliance with the recommendations for therapeutic intervention, particularly as it is not imperative that the physician follows the advice. In addition, regardless of the awareness of the NST, the rate of consultations have been reported as low, even in the ICU where patients are indicated for nutritional support [7,8]. To solve this problem, a message-window informing the physician that a patient is indicated for consultation with the NST was created in the electronic chart of patients in the hospital, after which consultation rates increased. However, nutritional support strategies were different for patients depending on a physicianŌĆÖs preference. Therefore, physiciansŌĆÖ compliance was the focus of this study which was compared with several outcomes such as nutritional variables and the results of treatment between the compliance group and the non-compliance group. In the compliance group, the supply and target performance rates of calories as well as the supply of protein after the NST consultation increased significantly. The compliant group, who had interventions recommended by the NST followed by the physician, showed a similar tendency to other studies [9,17]. Without the NST intervention, attending physicians may not be interested in nutritional therapy or the supply of calories and proteins possibly due to the lack of education, over-working, or manpower [18,19]. The rate of consultation was only 39% in a university hospital in Korea in 2015 and it was variable depending on the department [20]. According to a survey conducted in 2012, about 80% of attending physicians in Korea knew of the existence of the NST in their hospital, but this rate did not correlated with the rate of consultations with the NST [7]. It is important to increase individual awareness about the NST to increase physician compliance with NST recommendations.
In this current study, the compliance group received more calories and protein. An adequate supply of calories and protein for critically ill patients has been emphasized. Such patients are often under stressful conditions such as negative balance of nitrogen. Therefore, protein should be supplied to these patients successfully [3]. In addition, the closer to the goal of total calorie intake and protein intake, the lower the duration of hospital stay, and the greater the survival rate [21]. However, it is very difficult to take such a goal into practice in the ICU. In the 2000s, it was observed in Europe that the average supply rate of calories was 40% to 50% of the goal [15,22,23]. In 2010 in the ROK 52% of patients were supplied with the adequate amount of calories, reaching 80ŌĆō100% of the goal [16]. In 2015ŌĆō2016 in this current study, the total calories given to all patients reached 50ŌĆō60% of the goal before consulting with the NST. After the consultation, the compliance group reached 80% of the goal, while the non-compliance group reached 59% of the calorie goal. It appears that many patients do not get adequate nutritional support without the NST recommendations. Interestingly, there has been reports regarding underfeeding (80% of total energy requirement) which have emphasized the positive effects of ICU treatment compared with full feeding which is similar to total energy intake of the compliance group in our study [24,25].
The method of delivery of nutritional support is also important. Furthermore, enteral nutrition has been regarded as a preferred method of nutritional support because the intestine is regarded as an immune organ as well as a digestive organ. If the gut is not used for a long time, the mucosal barrier may break down, making it easy for gut bacteria to penetrate the blood stream [3,26]. In addition, parenteral nutrition is expensive and is also correlated with infection [3]. However, parenteral nutrition is still a commonly used method in Korea [27]. Therefore, the NST plays an important role in reducing the prevalence of parenteral nutrition. This has been observed in this current study, and is similar to results of other studies [10,27].
The compliance group had a better survival rate than the non-compliance group in the beyond 1 year-follow up after the NST consultation. After survival curves were adjusted by age, gender, weight and APACHE II score, the result was similar (hazard ratio: 2.21, 95% CI: 0.97ŌĆō5.02; Figure 2). Of course, outcomes of treatment cannot be considered only by nutritional resources. However, it is valuable to have observed that there are definite differences in terms of nutritional strategies between the compliance and non-compliance groups. The compliance group had an increase in the supply of calories and amount of protein and so had a greater accomplishment rate of the goals after a consultation with the NST. This might be a reason for the observed survival benefit. The attempt to meet the calorie target has been associated with improved outcomes in critically ill patients in a previous study [25].
This study had several limitations. Firstly, the data were collected retrospectively in this study. There were a lot of different characteristics between the 2 groups. After representative risk factors were adjusted before analysis, outcomes including death rate were still influenced by many factors, especially in critically ill patients. In addition, many consultations were requested in the first week following admission. Nutritional factors have a lower priority than medical treatment or resuscitative procedure to influence patient outcome in the ICU [25]. Therefore, cases of death within 2 weeks after consultation with the NST were excluded from analysis in this study.
Critically ill patients whose attending physician complied with the NST advice received an increased intake of calories and protein supply, and achieved a better target supply level than patients in the non-compliant group. In addition, the survival rate of the compliance group was higher than the non-compliance group beyond 1 year after the NST consultation. For this reason, compliance with the recommendations proposed by the NST by the attending physician is needed to increase the survival rate of critically ill patients. Further investigations are needed to confirm these results in the future.