Uncommon Mechanism of Mangled Extremity; Three Cases of Rope Entanglement Injury of the Lower Leg
Article information

Abstract
Rope entanglement injury is a rare entity. Previous reported studies mainly consisted of finger-related injuries. We describe three cases of rope entanglement injury of the lower leg. In the first patient, a below-the-knee amputation was performed as the primary treatment for unilateral amputated lower limb. In the second patient, a below-the-knee amputation and perineal wound management were simultaneously performed. The third patient had vascular injury combined with internal soft tissue injury without related bone fracture. He suffered serious sequelae from a delay in transfer from a local hospital. Rope entanglement injuries of the lower leg do not present in a consistent manner, and the treatment of accompanying injuries should be considered from an early stage. Care should be taken to ensure that there are no internal injuries missed because the exterior appears to be stable.
Introduction
Rope entanglement injury is a rare entity. It is usually caused by the application of a linear force to a small area which results in the tearing of the body part which was trapped in the rope [1–3]. Rope entanglement injuries are mainly reported to be related to finger injuries, and are known as injuries related to extreme sports or recreational activities such as climbing, waterskiing, and rodeos [1–6]. Injury could present in a variety of ways, from simple superficial injuries to tissue avulsion and amputations [1,2,5,6]. The type of rope entanglement injuries that occur in environments with high-energy transmission of force, where thick strong ropes are used, expose the person to trauma. These rope injuries could take the form of a mangled extremity. This describes injury to three or more of the four systems of soft tissue, bone, nerves, and blood vessels [7]. In this study, three cases of rope entanglement injuries of the lower leg are described to share the lessons learned from each case and case comparisons.
This study was approved by Institutional Review Board of Ulsan University Hospital (no.: 2021-06-023).
Case Report
In Case 1, a 36-year-old male patient presented needing a below-the-knee amputation of his right leg (Figure 1). The patient suffered trauma, whilst working on the deck of the ship, due to the rope wrapping around the patient’s right calf. Shortly after the accident, he was taken to our trauma center via emergency medical service and it took 36 minutes from the scene of the accident to the emergency room at Ulsan University Hospital. At the time of arrival, the patient’s vital signs were within the normal range, and there were no abnormalities in the vital signs during the resuscitation process. In the emergency room, temporary hemostasis was performed by applying a tourniquet to the ipsilateral thigh. Considering future rehabilitation and return to daily life, the ipsilateral thigh was targeted to prevent the need for an above-the-knee amputation. As a result, the below-the-knee amputation was successfully performed. However, due to lack of skin to cover the surgical site, the stump had to be managed in collaboration with a plastic surgeon. The patient had no additional vascular or orthopedic complications and was discharged after hospitalization for three months (including a three-week rehabilitation period).
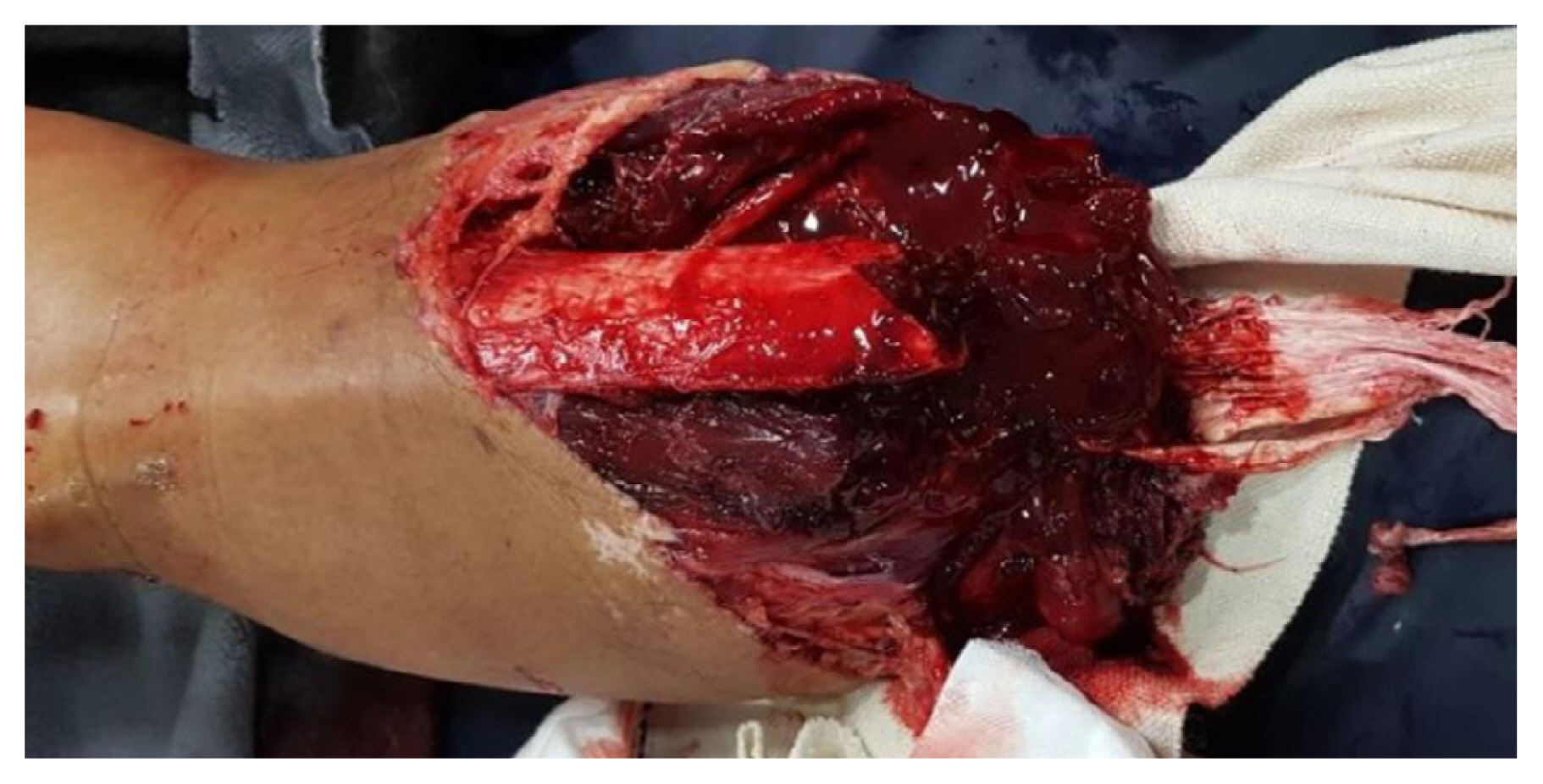
Initial findings of injured lower limb in Case 1. Exposed fractured bone with disrupted soft tissue with bleeding.
In Case 2, a 30-year-old male patient presented requiring a below-the-knee amputation of his left leg. The patient was wounded by a rope whilst working on a marine vessel 40 km away from the port, and the port was 33 km away from our trauma center. He was transported to our hospital by an emergency medical service air transport helicopter. It took 94 minutes from the scene of the accident at sea to the emergency room. He was wounded by a thick rope and then thrown into the sea by the moving force of the rope. At the time of arrival, the patient’s vital signs were checked. He had a systolic blood pressure (SBP) of 125 mmHg, a diastolic blood pressure of 73 mmHg, a heart rate of 123 bpm, a respiratory rate (RR) of 20 breaths per minute, and a body temperature of 35.9°C. About 9 minutes after arrival, the patient’s SBP dropped to 78 mmHg, and it was restored to within the normal range through the rapid transfusion of three units of packed red blood cell. The patient presented with major damage to the area where the rope was entangled, and the ipsilateral inguinal and perineal area were also injured where the torso and lower extremity were connected. This area, the transitional zone, was pulled by the rope when he was catapulted into the sea (Figure 2A). The perineal wounds were associated with open pelvic fractures (Figure 2B), and the wounds were managed by applying continuous negative pressure wound therapy (Figures 2C and 2D), and a diverting S-loop colostomy was performed to prevent wound contamination. At the same time, urethra rupture was confirmed during resuscitation, and open tube cystostomy was performed in the emergency room. Following this, primary urethral anastomosis was performed simultaneously with orthopedic and abdominal surgery. After 38 days of hospitalization (including rehabilitation), he was discharged; continued intensive rehabilitation was needed at the specialized hospital. The S-loop colostomy take-down was successfully performed 6 months later. There were no additional vascular or orthopedic problems following the primary surgery.

Initial findings of concomitant injuries in Case 2: (A) soft tissue transition zone at the ipsilateral side of the injury; (B) computerized tomography image of the fractures of the right pubic inferior ramus, ischial body, and ischiopubic acetabulum; (C) findings two days after the initial surgery; and (D) findings eleven days after the initial surgery.
In Case 3, a 68-year-old male presented with pain and discomfort in the right lower leg; three days prior to this the patient had been admitted to a local clinic with swelling and bruising all over his right leg. A rope had tightly wrapped around his knee whilst working on the deck of a ship (Figures 3A and 3B). At the time of admission to our hospital the patient’s vital signs were checked, he had a SBP of 145 mmHg, a diastolic blood pressure of 65 mmHg, a heart rate of 110 bpm, a respiratory rate of 18 breaths per minutes, and a body temperature of 38.7°C. He complained of coldness, decreased sensation and movement in the below-the-knee area. In physical examination, traces of rope wrapping from the popliteal fossa to just above the patella were observed. In addition, there was coldness, and decreased sensory and motor function that were clearly divided into upper and lower parts of the leg from the traces performed. Sensory function was decreased below the knee, going through the ankle to the toes, and motor function deficit was observed at the ankle, below the ankle, and included the foot-drop. A partial thrombus formation at the distal superficial femoral artery and arterial occlusive signs in the popliteal artery were confirmed using computed tomography angiography (Figure 3C). Distal outflow was weak, and soft tissue swelling of the entire right lower extremity, including the thigh, was observed. The ischemic time was over 72 hours and the mangled extremity severity score (MESS) was calculated as 12. The surgery was performed using the posterior popliteal approach in prone position. Surgical findings showed partial thrombus formation in the distal superficial femoral artery to the upper third of the popliteal artery connecting the dissected popliteal artery segment (Figure 4A). A vertical arteriotomy was performed perpendicular to the dissected segment, then a proximal and distal thrombectomy, fissured intima approximation, and bovine patch angioplasty for storing intima lining was performed sequentially (Figure 4B). The operation was terminated after confirming that the pedal pulse had recovered in the operating room by using Doppler ultrasonography. A prophylactic calf 4-compartment fasciotomy was performed considering the high probability of compartment syndrome occurring. In the process of improving the swelling, we worked with a plastic surgeon to remove the devitalized soft tissue, applied continuous negative pressure wound therapy, and performed a skin graft to manage the wound. The patient was discharged after 80 days of hospitalization (including rehabilitation), and there were no additional complications related to circulation during treatment.

Initial findings of injured lower limb in Case 3: (A) gross anterior view of the injured limb; (B) gross posterior view of the injured limb; and (C) right popliteal artery occlusion was observed in the lower leg on computerized tomography angiography
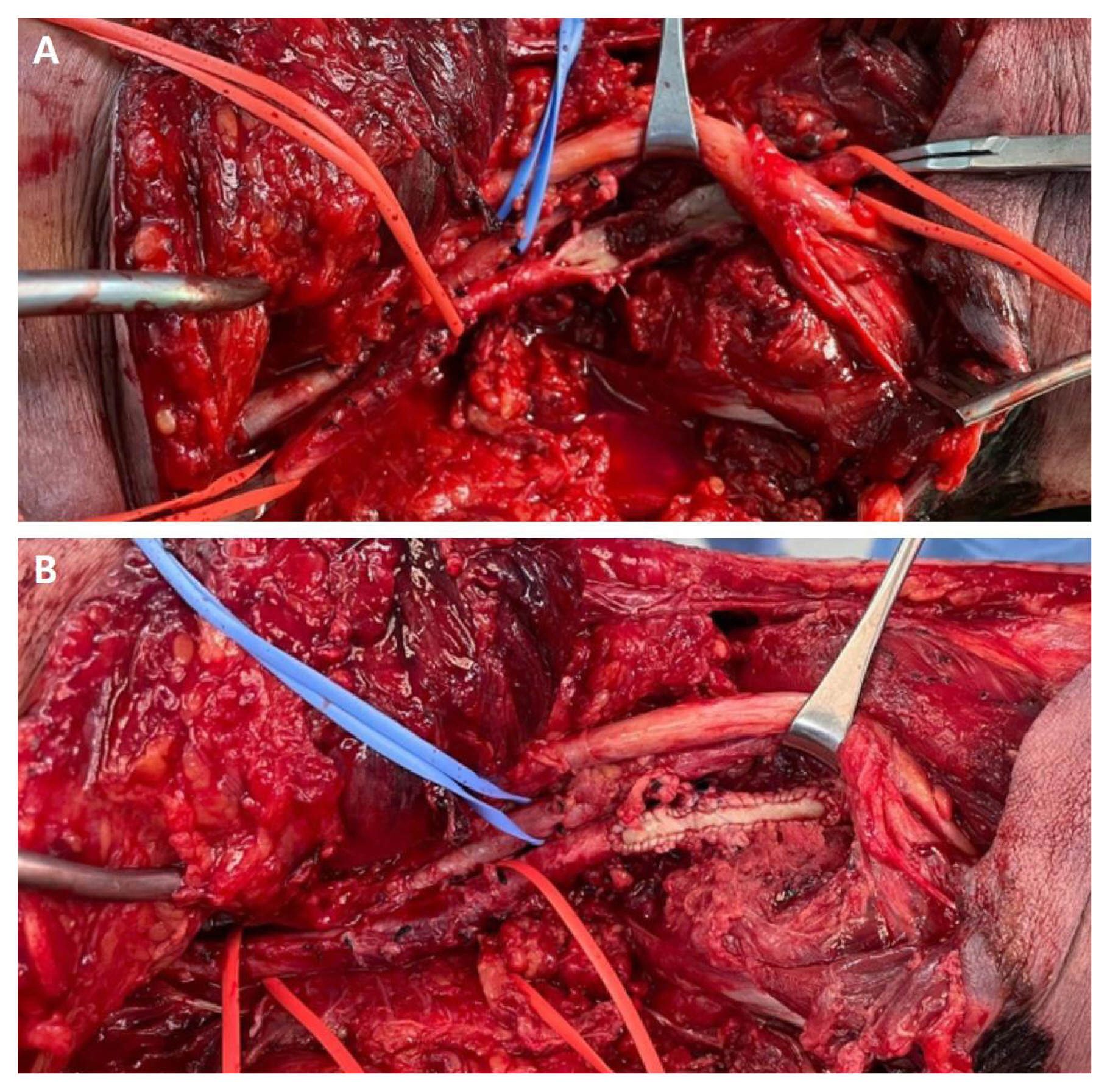
Surgical findings of damaged popliteal artery in Case 3: (A) the exposed intima of the dissected popliteal artery from the inside; and (B) after popliteal artery plication with bovine patch angioplasty.
Discussion
In the first case, a force strong enough to amputate the leg at the moment of the rope winding around the leg. In the second case, an additional proximal injury occurred due to the traction and counter-traction effect which occurred at the same time as the transmission of the same force described in the first case. In the third case, the leg was not amputated, but an internal degloving and neurovascular bundle damage occurred due to the force of transmission at the moment of winding of the rope (Table 1).

Summary of patients with lower extremity rope entanglement injuries.
The concept of rope entanglement injury originated from the experiences gained from climbing accidents [5,6]. It is considered to be mainly due to the various situations that can occur during the fall phase whilst using ropes [5,6]. Although there are no reports of the exact mechanism causing serious damage, it is presumed that crushing injuries are caused by the transmission of shearing forces when knots do not unwrap [6], and these injuries could occur in the lower extremity of the body as a form of high energy transmission.
In the city of Ulsan, where our trauma center is located, these types of injuries occur due to the geographical nature of city which is both coastal and industrial. Since the National Designated Regional Trauma Center in Ulsan opened in 2014, there have been three patients with lower leg rope entanglement injury. All three patients had the entangled rope injury in one lower limb, and the damage was in the form of severe tissue destruction due to strong force and high energy transmission. The strong force was caused by entangled rope which maximizes tissue destruction, and can cause amputation-type damage.
In the Case 2, the perineal wound probably occurred as the traction and counter-traction effect, transmitted in the transitional zone area, at the same time as the elastic potential energy was raised when the leg was wrapped in the rope and the patient was thrown into the sea. Although there were no clear reports on the damage mechanism of the same pattern, similar force transmission could be inferred in bungee jumping. At the lowest point phase of the bungee jump, the downward plunge is converted into an upward motion when the rope reaches its elastic limit. At that point, the forces are transferred to the effect opposite to traction. This strain of force can cause a traction and counter-traction effect that is transmitted to the jumper’s body, which can result in traction injuries [8–10]. Reports of peroneal nerve injury and femur fractures during bungee jumping could be explained by these types of forces [9–11].
In traumatic vascular injury, the golden time from injury to reperfusion is generally accepted as six hours [11–13]. More recent studies have reported that, in addition to damage control, concepts such as temporary intravascular shunt, and faster reperfusion strategies to vascular injury are needed [14,15]. MESS was designed to determine the initial evaluation and treatment decision of mangled extremity. It is based on the mechanism of injury and the degree of accompanying soft tissue injury, the status of ischemic change and ischemic time, the presence and status of shock, and age [12,13]. There are various opinions on clinical practice and interpretation of this scoring system [16,17], but it is helpful in understanding overall patient status. In Case 3, more than 72 hours of ischemic time elapsed, and the MESS was evaluated as twelve. Nevertheless, limb salvage was successful without additional procedures or vascular problems. Since the functional status has deviated from a certain level due to ischemic changes from the time of visiting our trauma center, it is difficult to apply the functional status to the evaluation of our practice. At the stage of primary care or whilst in hospitals that do not have a suitable environment for trauma treatment, timely transfer of these patients to a suitable trauma center is mandatory [18,19]. It is evaluated that treatment at a suitable institution where definite treatment is possible at the initial stage of the injury was urgently needed.
In Case 3, soft tissue damage in the form of a degloving injury and vascular damage were present. Neurological symptoms below the damaged area could be also regarded as ischemic nerve damage due to blood flow disturbance, but it was considered that the possibility of traumatic nerve damage that was accompanied at the time of the injury could not be completely ruled out. So, by definition [7], it was included in the category of mangled extremity.
According to the characteristics of this study cases that occurred in the marine environment, there were concerns about potential wound problems which may be caused by certain infections such as Vibrio and Clostridium species, Aeromonas hydrophilia, Pseudomonas species, Mycobacterium marinum, Erysipelothrix rhusiopathiae, and other microbes that are rarely seen in typical land-based, soft tissue injuries with open wounds [20]. However, in all three patients, no microbes were identified in the initial and repeated studies, and there were no problems with the selection of antibiotics related to wound infection or microbe identification.
Rope entanglement injuries of the lower leg rarely occur but are noteworthy. These injuries accompanied by high-energy transmission should be actively considered for timely transfer to a suitable trauma center. In the clinical situation, rather than focusing only on the main injury site, the possible harms and concomitant injuries should be considered according to the mechanism and circumstance of injury. There are also reasons to suspect serious hidden injury, even if the wound at first appears to be visually stable.
Notes
Author Contributions
Study conceptualization: NM and KJ. Validation: KKH and KS. Investigation: NM, CS and KJ. Manuscript writing: NM and CK. Manuscript review and editing: KS, KMA and KJ.
Conflicts of Interest
Jihoon Kim is an editor of Journal of Acute Care Surgery but this had no influence in the decision to publish this article. No other potential conflict of interest relevant to this article was reported.
Ethical Statement
This research did not involve any human or animal experiments.
Data Availability
All relevant data are included in this manuscript.
Funding
None.