


Introduction
In 2015, the law to restrict the working hours of medical residents called ŌĆ£the act to improve training conditions and the status of medical residentsŌĆØ was discussed. In Korea, ŌĆ£hospitalistsŌĆØ were introduced as a countermeasure for the shortage of doctors [1]. The demand for hospitalists has increased because the quality of medical care has decreased due to the shortage of hospital doctors. This resulted from the transition of internal medicine residents to the three-year system, the decrease in patient satisfaction, and the systematization of the education of residents due to the lack of time training [1,2]. Since the introduction of the hospitalist under a pilot project of the Korean Ministry of Health and Welfare implemented in 2016, the number of hospitalists has increased every year, and the number of patients that are under the care of hospitalists has continued to increase [2]. In January 2021, the hospitalist role was formally implemented. However, the proportion of hospitalists is on the decline due to inflexible government operational methods [3].
In the United States, the hospitalist system was first conceived by an inpatient management specialist in obstetrics and gynecology in the 1990s. Since then, it has been implemented and maintained for about 30 years, establishing itself as hospital medicine. The American Society of Hospital Medicine reported that approximately 48,000 hospitalists were employed in the USA in 2018 [4ŌĆō7]. In addition, because of a shortage of emergency surgery specialists due to the various subdivisions of general surgery, and as the working hours restrictions for medical residents were fully implemented in 2003, a surgical hospitalist model was conceived. Based on this model, the main task of the surgical hospitalist was emergency surgery, emergency patient management, and performance of additionally requested surgery. It was reported that the application of this model reduced the time required for emergency surgery and increased the income of the general surgery department [8]. However, this concept is different from the work of a hospitalist who majored in hospital medicine, and in 2017 when it merged with trauma surgery, and changed to ŌĆ£acute care surgeryŌĆØ [9,10].
In Korea, in line with the change of the three-year resident training system, the department of surgery applied a pilot project utilizing hospitalists in order to assess hospital costs and postoperative outcomes [11]. In the Department of Surgery, due to the nature of surgical treatment, the reduction of the training period and limitations associated with working hours are becoming a problem not only in the absence of treatment, but also in terms of the training of specialized surgeons [12,13]. Recruiting surgical hospitalists (if the hospital can fill the position), presents several difficulties. In this review the difficulties of being surgical hospitalists, and the limitations related to their recruitment will be reviewed, and we will introduce the new model of surgical hospitalist which was implemented at our institution.
Difficulty in Applying the Surgical Hospitalist Role
Currently, for the hospital to receive the hospitalist fee-for-service in Korea, the hospitalist system must be operated in the same way regardless of the department. However, the detailed model of each department is operated differently depending on the institution. Although it is advantageous for surgeons who have knowledge of physiological changes and perioperative management following surgery to act as surgical hospitalists, there are several difficulties in performing the role of a surgical hospitalist. Firstly, there is no reference model. Although five years have passed since the pilot project was implemented, surgical hospitalists in different hospitals operate in very diverse ways. Moreover, under the current fee-for-service system, the hospitalist system is operated mainly in large hospitals with sufficient human resources infrastructure [1,11]. In 2021, the total number of surgical hospitalists increased, but recruiting hospitalists in small and medium-sized hospitals or hospitals in provincial cities has remained challenging. Secondly, there is a special relationship between the operating surgeon and the patient. Since patients have a special rapport with the doctor who directly operates, the surgical hospitalist emphasizes the assistant role to the surgeon as opposed to a professional decision-making position. In addition, when complications occur after surgery, there are difficulties for a primary care physician due to the problem of responsibility, therefore making it difficult for surgical hospitalists to make independent decisions. Finally, there is ambiguity in the division of roles between surgical hospitalists and medical residents. However, in most hospitals, the role of the resident has been replaced by the hospitalist who may not have the expertise or knowledge for making key decisions for the management of moderate-intensity patients [4,6,11].
Reasons for Low Hospitalist Application Rate Among Surgical Residents
There are several reasons explaining why surgical residents do not prefer to become hospitalists after training, despite the relatively high wages and the rest time from surgery guaranteed. Firstly, if a surgical resident chooses the hospitalist path right away, they cannot operate. However, unlike internal medicine, surgeons require time to develop specialized surgical skills. Therefore, if a surgical resident chooses a hospitalist role immediately after training, it becomes difficult for them to gain experience in specialized surgery. A 2nd reason is the instability of employment and lack of professionalism towards hospitalists. Since most surgical hospitalists are non-regular workers requiring high wages, hospitals are expected to influence wages by hiring hospitalists. This compels hospitalists to pursue maximum patient care to preserve labor costs. However, this can potentially result in treating mildly ill patients, rather than the in-depth treatment of critically ill patients requiring specialization. In addition, because the scope of hospitalist treatment is ambiguous and the professional education program insufficient, it is difficult to guarantee the competencies of the occupational group. Ultimately, this fosters anxiety about the employment of hospitalists. In this context it is difficult for a surgeon to give up surgery.
Composition of the Admission Critical Care Trauma Surgery Team
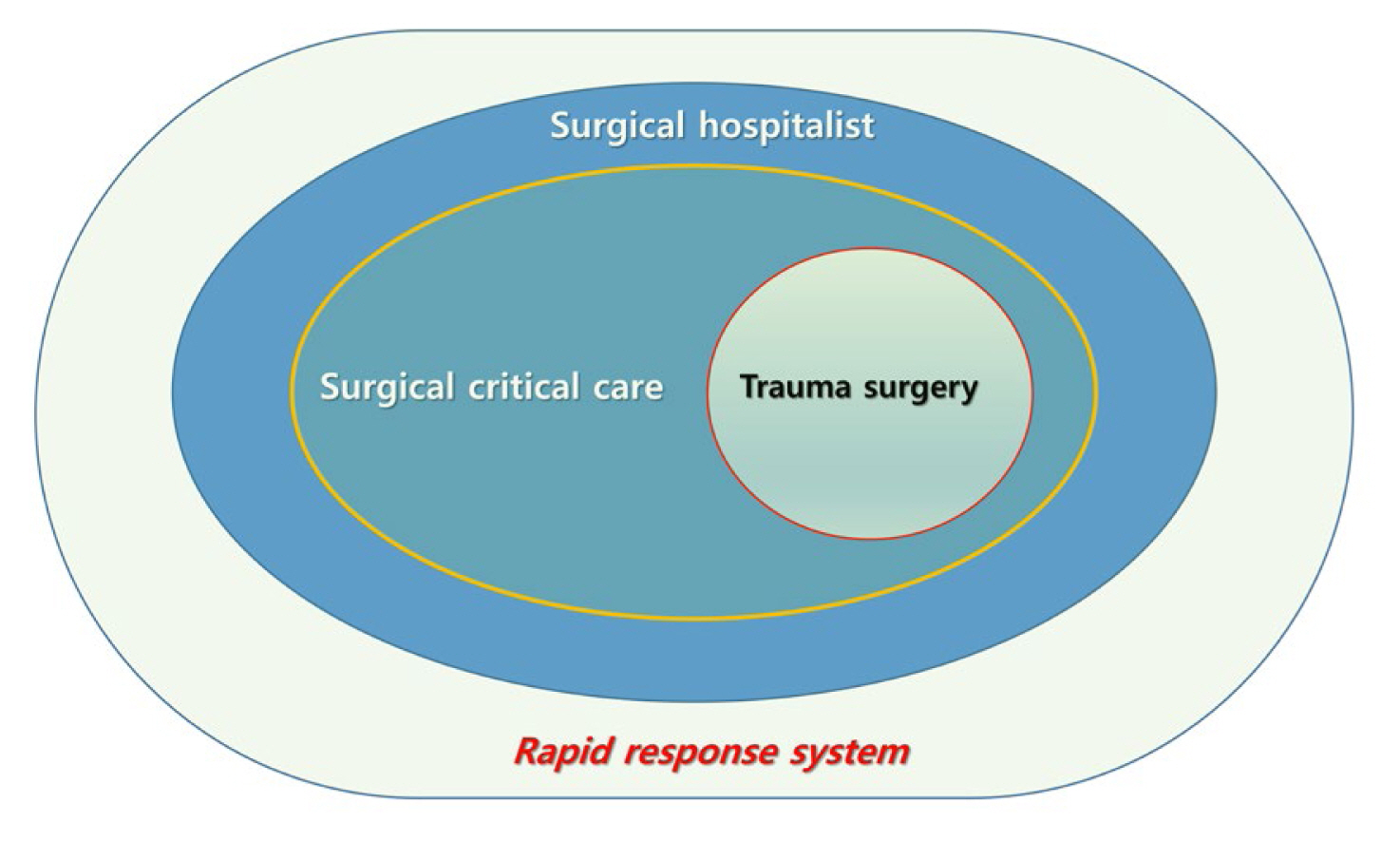
Since the late 2000s there have been concerns in the United States related to the deterioration of the quality of care for emergency surgery patients, due to the subdivision of the surgical divisions and the enforcement of the Act on Restriction of Working Hours for Medical Residents [8]. As a countermeasure for this, the concept of surgical hospitalist was devised [8]. The characteristics of a surgical hospitalist are different from those of a medical hospitalist who practices general hospital medicine [1,6,8]. Surgical hospitalists were joined by trauma surgeons specializing in intensive care and developed into the concept of acute care surgery (ACS) by combining acute abdomen care, critical care, and trauma care [8ŌĆō10]. We devised the concept of admission, critical care, and trauma surgery (ACTs) by combining the concepts of medical hospitalist, except for acute abdomen care in ACS. The core of ACS or ACTs is critical care and trauma management, and depending on the circumstances of each institution, it can be applied flexibly to ACS if an emergency surgery part is operated and ACTs if a surgical hospitalist is operated.
The ACTs team is a surgical team composed of specialists in intensive care and trauma surgery that manage critically ill patients in the surgical ward and in the surgical intensive care unit (ICU). Therefore, to fully demonstrate competency as a surgical intensivist, management is focused on patients with severe disease who do not undergo a general course after surgery, or on patients with a potential for severe conversion. In 2021, the National Health Insurance Service Ilsan Hospital Department of Surgery had two intensivists on duty once a week, that were in charge of the ICU after regular hours, were responsible for the back-up of critically ill patients in the ward, and served as an immediate response to trauma patients visiting the emergency room. In addition, the ACTs team conducts in-hospital rapid response team (RRT) activities. Furthermore, it utilizes a severity screening program to preemptively identify patients with a high probability of being seriously ill, and a national early warning score (NEWS) score of 5 or higher in the surgical ward. Patients screened by the ACTs team undergo back-up in the ward or are transferred to the ICU (Figure 1).
Specific Operation Plan of the ACTs Team
The ACTs team can have a flexible operating method depending on the number of its members. The minimum number of members who can cover 24 hours and 7 days is 5ŌĆō6 people. In this case, 5ŌĆō6 working days per person per month are covered. During regular hours, at least one surgical intensivist, 2ŌĆō3 surgical hospitalists, a surgical ward rapid response team screening, one trauma duty, and full-time watchers are off work. Currently, four people operate the ACTs team: one surgical intensivist, two surgical hospitalists, and a surgical ward rapid response team screening. In addition, the duty is implemented 3 days a week (Table 1). However, if the ACTs team is a 6-person system, an alternative operation mode is possible by dividing the week into 14 sessions of 12 hours each. These can then be further divided into 5-day and 9-night and weekend sessions, in the form of one intensivist, two hospitalists, and one working night shift, with three people covering day sessions 5 times, and the remaining three people covering night and weekend sessions 9 times (Table 1).
After reviewing all patients admitted to the care of the ACTs team at the morning conference, surgical ICU, emergency ICU, rapid response team screened patients, and general surgery ward critically ill patients, the morning round is then performed. After that, the ACT team meets again in the afternoon after work to proceed with the change of patients and the transfer of duty hours. In addition, the ACTs team conducts critical care conferences with specialists from respiratory medicine, anesthesia and pain medicine, cardiology, and surgery every week, journal review, patient review through the trauma and emergency surgery conference, and panel discussion for evaluation of trauma related preventable deaths twice a year. In addition, the rapid response team conference is conducted to evaluate the involvement of surgical patients before they worsen. The ACTs team also participates in the nutrition support team conference for evaluating the nutritional status of ward patients as well as of patients in the surgical ICU, and discuss nutrition improvement plans with nutritionists, nurses, and pharmacists (Table 2).
Advantages of the ACTs Team
One of the strengths of the ACTs team is that the autonomy and independence of hospitalists are maintained. It is safe to say that the current hospitalist system is a ŌĆ£designated ward-only doctor.ŌĆØ According to that, a hospitalist is forced to provide only treatment within their designated ward. In addition, since revenue is generated according to the number of patients, hospitals are encouraged to treat as many patients as possible. This may lead to problems in that hospitalists may focus on treating patients with mild conditions. Emergency situations and critically ill patients do not only occur in designated wards. Moreover, emergency patients in non-designated wards can be in an even more dangerous situation if the response is delayed or insufficient.
The ACTs team is freed from the restrictions tied to the designated ward, it provides back-up for all patients in the surgical field who need intensive monitoring, and can directly respond to emergencies. Secondly, it can have flexibility in the operation of the ICU. Currently, under the Korean medical insurance reimbursement system, intensivists in the ICU are restricted from treating patients in general wards. Among patients transferred from the ICU to the general ward, patients who need short-term intensive monitoring or do not have follow-up surgeons are transferred to the ACTs team. The new ACTs model will help the surgical department to receive reimbursement for ICU intensivists. In addition, it can support the management of critically ill patients during the acute period after leaving the ICU. Hospitals focused on trauma may not be able to charge an intensivist fee for the treatment of trauma patients in a general ward. However, the ACTs team, which is composed of acute care surgery specialists, incurs an intensivist fee. When a patient is moved from the ICU to a general ward, the patient is transferred to a hospitalist, who is a trauma specialist, to ensure continuity of treatment. Thirdly, the ACTs team operation is expected to improve patient safety through continuous screening and preemptive measures for patients with the potential for exacerbation. The active involvement and back-up for all surgical patients by the ACTs team are thought to have played an essential role in reducing the incidence of CPR per 1,000 hospitalized patients from 0.81 to 0.55 between 2019 to 2021 (Table 3). Fourthly, the expanded operation of the ACTs team is expected to lead towards the establishment of a 24-hour specialist management system for patients. Currently, four ACTs team specialists perform in-hospital night duty once a week. These teams oversee treating patients, both in the ICU and general ward, with a high possibility of an exacerbation. Therefore, if enough staffing is secured for the ACTs team, it will be possible to build a system that covers nights and holidays, which is expected to maximize patient safety.
Early Experience of Operating of the ACTs Team
From March to December 2021, the ACTs team treated 101 (63.9%) patients out of 158 surgical patients admitted to the emergency ICU. These consisted of 62 critically ill surgical patients (61.3%), 29 patients with severe trauma (28.7%), and 10 surgical patients (9.9%) who were treated in the ICU through RRT screening. Among them, 14 patients (13.9%) died. A total of 2,049 cases were screened by the RRT in the surgical ward and reviewed, and involved in the ACTs team, in the order of general surgery, orthopedic surgery, urology, and plastic surgery. Of these, 10 patients were transferred to the ACTs team and underwent critical care (Table 4).
Significance of the ACTs Team in Terms of Operating the Hospitalist System
Currently, the Korean hospitalist system compels hospitals to allocate the maximum number of patients to the hospitalist, and thus hospitalists focus on patients with mild conditions. As a result, critically ill patients in the ward who need the competence of a specialist are left to the medical resident. In addition, if treatment is mainly focused on critically ill patients, the workload of the hospitalist will be excessively increased. One study showed that an increase in hospitalistsŌĆÖ workload leads to an increase in the patientsŌĆÖ length of stay [14]. Therefore, it is very important to set an appropriate workload while demonstrating the competence of a specialist. Furthermore, general surgery in Korea suffers from a chronic lack of resident recruitment, and as the awareness of patient safety increases, the need for hospitalists also increases. As mentioned above, surgical hospitalists are challenging to employ due to their specificity, and the recruitment of surgical hospitalists is not increasing as expected. In the case of local, small or medium-sized hospitals, the employment of hospitalists with intensivist qualifications is expected to bring benefits in terms of hospital operational efficiency and patient safety. In addition, it is expected that large hospitals that can meet the demands for staff, will be able to secure continuity of treatment, and improve patient safety by having a specialist system 24 hours a day, 365 days a year. Furthermore, activation of the ACTs team is expected to resolve the lack of expertise and uncertainty about the future, which is why surgical residents do not readily choose the hospitalist path. In addition, the employment of trauma specialists is thought to help revitalize low-level trauma treatment centers.
There are several difficulties in operating an ACTs team within the surgical hospitalist system. Firstly, sufficient staffing is required. At least 5ŌĆō6 specialists are necessary for this model to operate as a 24/7 specialist system, which is challenging to realize in small and medium-sized hospitals. In addition, if the hospitalist system is operated as an ACTs team, hospitalist fee-for-service cannot be received by the hospital due to various roles in the current fee system. In addition, the number of patients eligible for hospitalist care is much smaller than the maximum number of patients per doctor in the current hospitalist system, because the target of care for a hospitalist should be patients with a severe condition. Therefore, in terms of profit efficiency it is low. However, despite these limitations, the application of the ACTs team is meaningful, given it provided continuity of treatment and providing stability of treatment in a situation where the number of resident recruitments was gradually decreasing, and it was possible to avoid duplication in human resource management. In the future it will be necessary to discuss the effect of expanding the application of hospitalists and the ACTs team in relation to various issues, such as the decrease of surgical residents and the increased concerns regarding patient safety.